Published online 21 September 2011 | Nature 477, 390-393 (2011) | doi:10.1038/477390a
News Feature
Bombs' hidden impact: The brain war
Wartime explosions may be creating an epidemic of brain damage — and a major challenge for scientists.
 M. ROMANA/AFP/GETTY IMAGES
M. ROMANA/AFP/GETTY IMAGES
To Burt, the blasts he experienced in Afghanistan eventually became a kind of music. The detonation of C4 and other such military-grade explosives felt like extremely high notes — painful, yet over quickly. But blasts from bombs made out of fertilizer — a favourite of Afghan insurgents — were like standing next to a speaker at a rock concert: the dull bass thuds didn't necessarily hurt, but they would reverberate through his body like a wave, and stay with him for a long time afterwards.
They're with him still. Burt, who asks that his real name not be used, spent four months as a tactical adviser to a US military bomb-disposal unit in Afghanistan, during which he was within 50 metres of a detonating improvised explosive device (IED) more than 18 times. His sleeping problems began even before he left. So did the headaches, the ringing in his ears and the nausea. He started to forget things — a problem that got even worse after he returned home. Burt would find himself in a room in his house and wonder why he was there. One time, he told his wife they should try a new restaurant in town. She replied that they had eaten there with friends just a few days before.
As recently as two years ago, this constellation of symptoms might have been diagnosed as a classic case of post-traumatic stress disorder (PTSD), a psychological condition that can be caused by the constant stress of being in combat. But Burt, now on medical leave, blames those low notes. He is convinced that the body-shaking blasts did something to his brain. And many doctors, medical researchers and military officials have come to believe he is right.
The visible toll of insurgent-made IEDs has been awful enough. In the ten years since military operations began in Afghanistan and then Iraq, IEDs have killed more than 3,000 US and allied troops, and wounded roughly ten times that number. But many more troops have been exposed to multiple blasts and not suffered any visible physical injuries. Like Burt, they often report an array of symptoms, ranging from sleep disturbance to problems concentrating. And an increasing body of evidence suggests that the repeated concussions have left them with an invisible, subcellular-level form of traumatic brain injury (TBI) that not only impairs their day-to-day functioning, but also increases their long-term risk of developing neurodegenerative diseases.
"We've got a lot of guys out there that might be 30 years old that have been blown up a dozen times," says Kevin Kit Parker, a biomedical engineer at Harvard University in Cambridge, Massachusetts, who is conducting research on TBI. "And the risk that these guys are going to get a disease like Alzheimer's or Parkinson's is soaring."
The number of troops affected by this kind of silent TBI has already topped 200,000, according to the Defense and Veterans Brain Injury Center in Washington DC. A survey done by the Rand Corporation, a not-for-profit research firm in Santa Monica, California, suggests it could be as high as 320,000. The Pentagon and the US Department of Veterans Affairs, which are responsible for the health care of current and former troops, respectively, are getting worried about a potential epidemic of disability and dementia. The disorder also presents a major challenge for researchers.

No one fully understands what the blast waves are doing to the brain, explains Walter Koroshetz, deputy director of the US National Institute of Neurological Disorders and Stroke in Bethesda, Maryland. Thanks to mounting evidence from professional sports, he says, "it's been known for a long time that repetitive head injuries lead to chronic degenerative disease. But no one has really got a hold on how that happens." Worse, he says, coming up with an effective treatment, and not just alleviating symptoms, could take years: some 20 compounds and interventions have been tested in more than 50 trials in the past 30 years. "People just look at this field and turn around and run," Koroshetz says.
Playing catch-up
The good news is that the Pentagon has finally begun to put a high priority on understanding, diagnosing and treating these injuries. But, as officials there now admit, it is playing catch-up after too many years of ignoring the problem.
"The system of care was really in denial for the longest time," says Colonel Christian Macedonia, a physician with the US Army who serves as medical-sciences adviser to Admiral Michael Mullen, chairman of the Joint Chiefs of Staff. Partly this was just the culture of the military, says Macedonia: because most soldiers dazed by a blast wave seemed to recover very quickly — on the surface — the attitude was, "Hey, shake it off".
When the symptoms did begin to show, he says, troops with TBI were often misdiagnosed as having PTSD, which has similar symptoms. And veterans of Iraq and Afghanistan have all too often been exposed to physical and psychological traumas that could easily cause both.
“People just look at this field and turn and run.”
But most of all, Macedonia thinks that the reluctance to recognize silent TBI was "the ghost of the Gulf War" — the ongoing scientific controversy around the diffuse symptoms described by many troops who served in the 1991 conflict. Study after study has failed to identify a root cause for Gulf War syndrome, he says, so when people started coming forward with TBI — yet another constellation of complaints that could not be linked to a single cause — the frustrated military-medicine hierarchy just didn't want to hear about it.
That attitude didn't begin to shift until senior military leaders began to sense a dissonance between the official reports they were being given and what they saw when visiting injured troops. One crucial moment came in 2009 when Marine Corps commandant General James Amos toured Walter Reed Hospital in Bethesda, Maryland, and was introduced to a patient who said, with considerable effort, "General, I know who you are. I have a picture of you and I together in Iraq."
It turned out that Amos had a copy of the picture, too. It had been taken just two years earlier, when he had posed with a group of marines who had just survived an IED that had detonated directly under their vehicle. Thanks to the vehicle's advanced armour, all of them seemed unscathed. But this young man, a bomb-disposal expert, went straight back to work and was quickly exposed to several more blasts. His physical condition deteriorated rapidly, his life began to unravel and — after some difficulty getting the military medical establishment to recognize his TBI — he had been admitted to Walter Reed with severe neurological problems.
Amos describes the meeting as a seminal moment for him. "This TBI business is real, and we've got to get past the point of ignoring it," he recalls of his reaction. "We need to do something about it."
“This TBI business is real, and we've got to get past the point of ignoring it.”
Mullen was coming to much the same conclusion. Concerned that he wasn't getting a full picture of the brain-injury problem, he asked Macedonia to help organize a 'Gray Team' of researchers and medical professionals with combat experience to look at the realities of TBI on the battlefield.
The Gray Team (named after the brain's grey matter) made its first visit to Afghanistan in 2009, says Macedonia, and quickly concluded that Mullen's suspicions were well founded. Official reports had claimed that more than 90% of troops with concussion were being assessed with the 13-point Military Acute Concussion Evaluation (MACE). But when the Gray Team travelled to Afghanistan, the group found that the vast majority of medical professionals — in both large military hospitals and remote outposts — didn't even know what a MACE was. "Doctors couldn't tell you the first thing about it, even though they had all the training materials," says Macedonia. No one was enforcing the screening.
In parallel with the efforts of the Gray Team, the Defense Advanced Research Projects Agency (DARPA) and the Office of Naval Research were sponsoring a study that for the first time sought to understand how the brain is affected by blast waves, which may cause different injuries from the blunt-force trauma seen in sports injuries. The study focused on breachers: marines who specialize in using explosives to enter buildings. The first paper is only now going through review, but researchers say that they have found evidence of neurological impairment in the instructors, who have had long-term, repeated exposure to low-level blasts.
On 21 June 2010, guided in part by the breacher study, the Pentagon announced its first policies for identifying and treating people who may have TBI. Included were the first military-wide mandatory triggers for screening troops, including a rule that anyone within 50 metres of a blast had to be evaluated for signs of brain injury.
The research scramble
The Pentagon has also started to make up for its long neglect of brain-injury research. The Department of Defense's Congressionally Directed Medical Research Programs, one of the major conduits for medical-research funding, provided no money specifically for TBI or PTSD between 1999 and 2005. In fiscal year 2006, a small amount, US$3.7 million, went to PTSD, but TBI was not even listed as a research topic. In 2007, however, mounting reports of battlefield brain injuries persuaded Congress to allocate $150 million for TBI research, with another $150 million for PTSD research.
 The US military is experimenting with the use of electroencephalography during the baseline pre-deployment testing of its troops.J. ANDERSON/AP
The US military is experimenting with the use of electroencephalography during the baseline pre-deployment testing of its troops.J. ANDERSON/AP
That influx of money was enough to open the door to people such as Parker, one of the few medical researchers working on TBI who has combat experience. His research focus had been on cardiac cell mechanics. But in 2002, he served the first of his two tours of duty as an infantry officer in Afghanistan and began to see the effects of TBI on his fellow soldiers. The bombs then were still relatively small and unsophisticated — artillery shells hooked up to garage-door openers, for instance. But by the time of his second tour in 2009, troops were encountering 200-kilogram fertilizer bombs that could blow unarmoured vehicles to smithereens. As he puts it, only half jokingly, once people started trying to kill him with IEDs, "I figured I had better turn into some kind of neuroscientist".
In fact, Parker's first formal involvement with brain-injury research began when he attended a DARPA workshop on the subject in 2005. There he learned that one of the challenges was to understand the effects of an explosive blast on the brain. With his background in cell mechanics, Parker immediately began to wonder about integrins, receptors that mediate the cell's attachment to surrounding tissue. Could a blast wave damage them enough to disrupt the proteins' functioning?
The idea got a cool reception at first, says Parker, who is now a member of the Gray Team. "The community that does neuroscience and understands cell mechanics is non-existent," he says. "It's like if you're used to reading English and I hand you a paper in Mandarin Chinese: it's going to be kind of difficult." But a grant from DARPA allowed Parker and his group to develop an in vitro model to test his idea. And in July, his team published a paper showing that the idea is essentially correct: blast-induced brain injury sets off a cellular chain reaction that disrupts integrin signalling, impairing connections among the brain's neurons (M. A. Hemphill et al. PLoS ONE 6, e22899; 2011).
The increased funding has also led to progress towards a blood test for diagnosing silent TBI. Currently, clinicians can only infer the presence of such brain damage by cognitive-impairment tests. This means that, because the symptoms overlap with those of other disorders, brain-injury researchers can't always be sure about what they're measuring — and patients might not be receiving the most appropriate care. Now, after looking at a variety of proteins that seem to become elevated in the bloodstream after a brain injury, army-funded researchers tested two that seemed especially promising in small-scale, phase II clinical trials. Known as ubiquitin C-terminal hydrolase (UCH-L1) and glial fibrillary acidic protein (GFAP), they will soon be tested in large-scale, phase III trials.
Working independently of the Pentagon, Bennet Omalu, a forensic pathologist at the University of California, Davis, and the chief medical examiner for San Joaquin County in California, has started to look at veterans' brains for chronic traumatic encephalopathy. First identified in professional athletes involved in contact sports, this neurodegenerative disorder is believed to be caused by multiple concussions. In November, Omalu expects to publish what may be the first case study demonstrating chronic traumatic encephalopathy in a military veteran with silent TBI.
 Click for larger image.
Click for larger image.
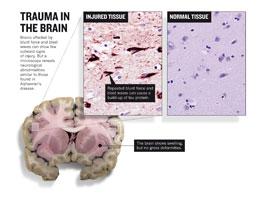
The young man had been exposed to multiple blasts during two deployments to Iraq, explains Omalu, who in 2005 published the first evidence of chronic traumatic encephalopathy, which he had identified from autopsy samples from an American football player (B. I. Omalu et al. Neurosurgery 57, 128–134; 2005). After returning home, the man began to experience memory problems, mood disorders and self-control problems. Then, aged 27, he committed suicide. With the permission of his relatives, says Omalu, "I got his brain, examined it, and lo and behold, he had CTE changes" — abnormal accumulations of the tau protein associated with Alzheimer's disease and other dementias (see 'Trauma in the brain').
Limited access
Few medical researchers working on brain injuries have an easy way to collaborate with the Pentagon. Its unique combination of bureaucracy and national-security considerations prevents access to many data and brain-tissue samples that could be useful for medical researchers. For example, access to the Pentagon's Joint Theater Trauma Registry — a compilation of all military trauma-related data — is highly restricted, lest enemies use the information to improve their ability to injure US soldiers. "Giving the NIH access is not impossible, but it is very, very difficult," says Major General James Gilman, who heads the US Army Medical Research and Materiel Command at Fort Detrick, Maryland.
There have been some signs of change. A joint programme by the US National Institutes of Health (NIH) and the Uniformed Services University of the Health Sciences, both in Bethesda, recently hired a neuropathologist specifically to look at brain tissue of deceased troops, although access to the tissue is not yet guaranteed. Also, the Pentagon and the NIH agreed in August to develop a database for TBI that is similar to the ones created for Alzheimer's disease, autism and cancer research. The idea is to standardize data collection across studies so that researchers can compare results more easily.
Among other things, such comparisons should help investigators to get a clearer picture of how well TBI therapies work. They need as much help as they can get, says Koroshetz: for all the progress in understanding the causes and progression of silent TBI, treatments remain elusive. Dozens of clinical trials have been done over the past two decades, looking at everything from antioxidants to hyperbaric oxygen. "No one has been able to figure out how to make a difference," says Koroshetz. "In terms of outcomes in patients, there is very little, if any, evidence that any single thing works."
The Pentagon has come a long way from just three years ago, when TBI was mostly ignored. In January, it became mandatory for the military to track all concussive injuries, and troops now receive pre-deployment cognitive testing that can be used as a baseline in case they are later affected by concussion. Experiments with brain-wave measurements are also under way. And with the new reporting requirements, the military is creating what is likely to be the single largest repository of data on TBI.
The question is how to keep the momentum going. That may prove difficult, given the United States' mounting budget woes. After the initial boost in 2007, funding levels for TBI research dropped dramatically. In fiscal year 2011, the congressional appropriation specifically for the Pentagon's brain-injury research is expected to be just $45 million. "Where's the interest, where's the support, where's the national effort?" asks Colonel Dallas Hack, director of the army's Combat Casualty Care Research Program at Fort Detrick.
ADVERTISEMENT

Brigadier General Robert Thomas, the army's assistant surgeon-general, hopes that the military's involvement is now doing for research and treatment of brain injuries what it has done in the past for yellow fever, trauma care and medical evacuation. For better or worse, he says, "combat is the greatest catalyst to medical innovation".
But in the meantime, Burt and the hundreds of thousands of other people with brain injuries can only hope that progress comes in time to help them. Once an ambitious multi-tasker, Burt says he now has problems with basic tasks. These days, he can get around the house, and even manage trips to the store — as long as he makes lists or uses some other form of reminder. "But I will never be what I was," he says.
See Editorial page 369
Sharon Weinberger is a Carnegie fellow at Northwestern University's Medill School of Journalism .
Comments
If you find something abusive or inappropriate or which does not otherwise comply with our Terms or Community Guidelines, please select the relevant'Report this comment' link.
Comments on this thread are vetted after posting.